Se habla español
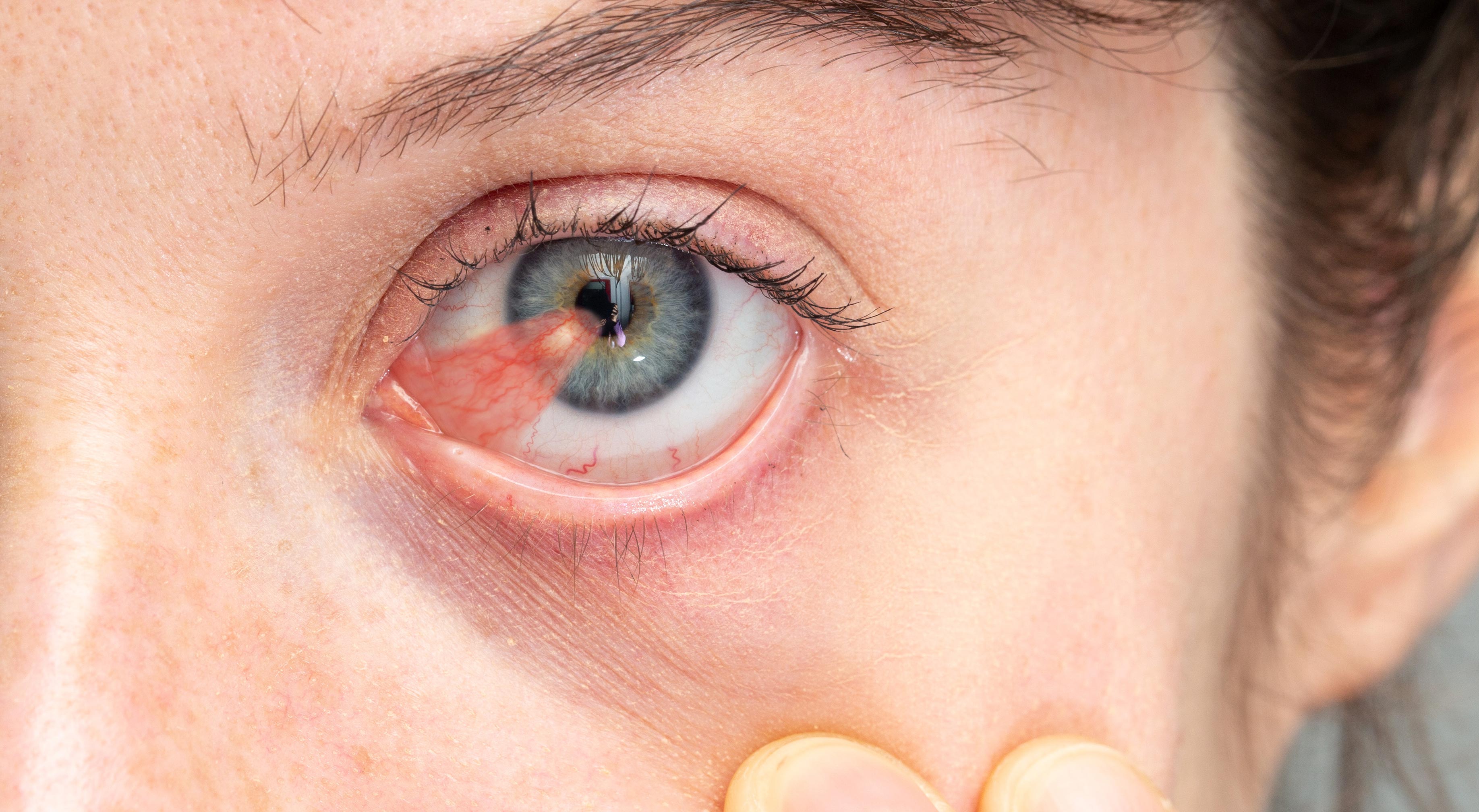
A pterygium is a triangular, benign growth of the conjunctiva that often advances onto the cornea. It typically starts on the white part of the eye near the nose and, over months or years, can creep inward toward the clear window that focuses light. Although not cancerous, these growths can interfere with comfort, tear film stability, and — in advanced cases — the quality of vision.
People who spend long hours outdoors in bright sunlight, wind, or dusty environments are more likely to develop a pterygium. Ultraviolet (UV) exposure is a major environmental driver, and geographic regions with intense sun or frequent airborne irritation see higher rates. Genetics and individual variations in the ocular surface response also play a role, which is why two people with similar sun exposure can have very different outcomes.
At Next Level Retina we approach pterygia with an emphasis on clear diagnosis, thoughtful prevention, and timely intervention when needed. Our goal is to preserve comfort and vision while minimizing the chance of recurrence after treatment.
Pterygia develop where the ocular surface is repeatedly stressed: UV radiation, wind, dust, chlorinated water, and chronic dryness all create an environment that promotes conjunctival overgrowth. The conjunctiva responds to this ongoing irritation by producing a triangular wedge of tissue that can migrate over the cornea. This reaction is thought to be a protective, though ultimately problematic, adaptation of the surface cells.
Risk factors include prolonged outdoor work or hobbies (farming, fishing, construction, certain sports), living in sunny climates, and inadequate eye protection. Age also contributes — pterygia most often appear in young to middle-aged adults and can progress over decades. Smoking and certain inflammatory conditions of the ocular surface may increase susceptibility as well.
Recognizing these risk patterns helps inform prevention strategies. Simple measures like high-quality UV-blocking sunglasses, brimmed hats, and strategies to control surface dryness can meaningfully reduce the likelihood of growth and slow progression when a pterygium is already present.
Many pterygia remain small and stable for long periods, causing only mild irritation or redness. When symptoms are present they often include a gritty or foreign-body sensation, intermittent tearing, and visible redness along the nasal conjunctiva. Because the growth alters the tear film, patients can experience fluctuating comfort and blurriness that improves with blinking or lubrication.
As a pterygium enlarges and encroaches on the cornea, it can induce astigmatism by changing the shape of the corneal surface. This distortion produces blurred or distorted vision that may not be correctable with glasses alone. In rare cases, a very large pterygium can directly obscure the visual axis and cause a measurable loss of acuity.
Regular monitoring is important to detect changes that threaten vision or comfort. Even small, asymptomatic lesions should be examined periodically because progression can be gradual and subtle until it becomes clinically significant.
Although pterygia are benign, some conjunctival lesions can mimic more concerning conditions such as conjunctival intraepithelial neoplasia or squamous cell carcinoma. A careful clinical exam evaluates color, vascular pattern, growth rate, and surface characteristics to differentiate benign from suspicious lesions. A rapidly growing, heavily pigmented, or nodular lesion may warrant further evaluation.
When the appearance is uncertain, your clinician may use slit-lamp photography and fluorescein staining to document surface changes, or recommend a biopsy for definitive histologic diagnosis. Early and accurate distinction between benign and malignant-appearing lesions is essential so that treatment can be appropriately targeted and timely.
Discussing the possible diagnoses openly helps patients understand the rationale for observation versus biopsy or excision. Accurate diagnosis minimizes unnecessary procedures while ensuring that anything that looks atypical is managed without delay.
Conservative management is the first line for many pterygia, especially those that are small and not threatening the visual axis. Lubricating artificial tears, nighttime gels, and topical anti-inflammatory drops for short courses can relieve irritation and improve ocular surface comfort. Addressing underlying dry eye disease or blepharitis often reduces the symptoms that prompt patients to seek treatment.
Preventive measures are equally important. Sunglasses that block 100% of UVA and UVB rays, wide-brimmed hats, and minimizing exposure to wind and airborne irritants can slow progression. For people with chronic surface inflammation, a tailored plan to manage inflammation and maintain tear film health can make a significant difference over years.
When conservative therapy controls symptoms and the lesion remains stable, ongoing observation with periodic photographs and examinations is a reasonable and often preferred approach.
Surgery becomes appropriate when a pterygium causes persistent discomfort, progressive astigmatism, or threatens the visual axis, or when cosmetic concerns are significant to the patient. Modern excision techniques pair careful removal of the abnormal tissue with autologous conjunctival grafting or amniotic membrane to reduce the risk of recurrence and preserve ocular surface health.
The procedure is typically performed in an outpatient setting with local anesthesia. Patients can expect temporary redness and mild discomfort for a few days, with most returning to normal activities within a week or two. Postoperative care focuses on inflammation control and infection prevention using prescribed drops, and follow-up visits ensure proper healing and early detection of any regrowth.
Recurrence rates have fallen with improved surgical techniques, though some patients remain at higher risk. Surgeons take individualized steps — such as using grafts and adjunctive therapies — to minimize recurrence and optimize cosmetic and functional outcomes.
A pterygium is a benign, triangular growth of conjunctival tissue that can extend from the white of the eye onto the cornea. It typically begins on the nasal side and progresses slowly over months or years, altering the ocular surface and tear film. Although not cancerous, larger pterygia can change corneal shape and affect vision.
The development is linked to chronic irritation of the ocular surface, with ultraviolet radiation, wind, dust and dryness as common triggers. The conjunctival cells respond to repeated stress by proliferating and creating a winglike wedge of tissue. Individual susceptibility varies, so similar environmental exposure does not produce the same outcome in every person.
People who spend significant time outdoors in bright sunlight, wind, or dusty conditions have a higher risk of pterygium. Occupations and hobbies such as farming, fishing, construction, and outdoor sports increase exposure to ultraviolet light and airborne irritants that promote growth. Living in sunny or arid regions further raises the likelihood of development.
Age and ocular surface health are also important factors, with pterygia most commonly appearing in young to middle-aged adults and progressing over decades. Chronic dry eye, prior ocular surface inflammation, and possibly smoking can increase susceptibility. Genetic factors influence how an individual’s conjunctiva responds to the same environmental stressors.
Early pterygia are often asymptomatic, but common symptoms include redness, a gritty or foreign-body sensation, intermittent tearing, and fluctuating vision. Patients may notice blurriness that improves with blinking or lubrication due to instability of the tear film. Cosmetic concerns or irritation that interferes with daily comfort are also valid reasons to seek evaluation.
You should seek prompt care if you experience progressive blurring, persistent pain, sudden changes in vision, or if the growth appears to be enlarging rapidly. These signs may indicate increasing corneal involvement or raise concern for an atypical lesion that requires further assessment. Regular monitoring helps detect clinically significant progression early.
Diagnosis is primarily clinical and performed with a slit-lamp examination to evaluate the lesion's size, vascular pattern, pigmentation and surface features. Typical pterygia have a triangular shape with fine, superficial vessels and a gradual leading edge on the cornea. Atypical features such as rapid growth, nodularity, heavy pigmentation or an irregular surface prompt further investigation.
When the appearance is uncertain, clinicians may document the lesion with slit-lamp photography, apply fluorescein staining to assess the surface, or recommend a biopsy for definitive histologic diagnosis. Distinguishing benign pterygia from conjunctival intraepithelial neoplasia or malignancy is essential to avoid delayed treatment of serious disease. Transparent communication about the diagnostic plan helps patients understand why observation, imaging, or tissue sampling may be recommended.
Many small or stable pterygia are managed without surgery using measures to improve comfort and address underlying ocular surface disease. Lubricating artificial tears, nighttime gels and brief courses of topical anti-inflammatory drops can relieve irritation and reduce redness. Treating associated dry eye or blepharitis often improves symptoms and decreases the rate at which patients seek more invasive care.
Preventive strategies such as wearing 100 percent UVA/UVB-blocking sunglasses, wide-brimmed hats and minimizing wind and dust exposure are recommended to slow progression. Periodic photographic monitoring allows clinicians to detect subtle growth or corneal encroachment over time. When symptoms remain controlled and the lesion is stable, continued observation is a reasonable approach.
Surgery is considered when a pterygium causes persistent discomfort, progressive astigmatism, encroaches on the visual axis, or presents significant cosmetic concern for the patient. Modern techniques focus on removing abnormal tissue and reconstructing the surface to lower recurrence risk, most commonly with autologous conjunctival autograft or amniotic membrane transplantation. Surgeons may also use adjunctive therapies to reduce regrowth in higher-risk cases.
The procedure is usually performed in an outpatient setting with local anesthesia and takes steps to preserve surrounding healthy tissue and ocular surface function. Expectations, risks and individualized decisions about graft choice and adjuncts are discussed before surgery. Careful intraoperative technique and postoperative management are central to achieving good cosmetic and functional outcomes.
After surgery patients commonly experience mild to moderate redness and a gritty sensation for several days, with gradual improvement over weeks. Most people can return to light activities within a few days, but full ocular surface healing and stabilization of vision and astigmatism may take several weeks to months. Postoperative care typically includes antibiotic and anti-inflammatory eye drops and scheduled follow-up visits to monitor healing.
It is important to follow activity restrictions your surgeon recommends, including avoiding eye rubbing and protecting the eye from sun and wind during early recovery. Using lubricating drops and attending follow-up appointments helps detect early signs of complications or recurrence. Communicating any sudden pain, vision loss, increasing redness or discharge promptly ensures timely intervention if needed.
Recurrence rates have fallen significantly with improved surgical techniques, but regrowth remains the most common postoperative concern. Using a conjunctival autograft or amniotic membrane and careful surgical technique are proven strategies to lower recurrence, and adjunctive therapies can be considered for patients with aggressive disease. Individual risk factors such as continued UV exposure, young age and chronic inflammation influence the likelihood of regrowth.
Long-term measures to reduce recurrence include strict UV protection, managing ocular surface inflammation and treating dry eye disease. Regular postoperative exams with photographic comparison help detect early regrowth when interventions can be most effective. A tailored plan based on each patient's risk profile offers the best chance of durable success.
Although most pterygia are slow-growing and nonemergent, urgent evaluation is warranted for sudden onset of severe pain, rapid vision loss, intense redness or signs of infection. Rapid enlargement, a new nodular component, or bleeding from the lesion are also reasons to seek prompt assessment. These changes may indicate complications or an atypical lesion requiring expedited care.
If you experience acute symptoms, contact your eye care provider or the office for same-day guidance to determine whether urgent in-person examination is needed. Early evaluation helps differentiate benign progression from conditions that require immediate treatment. Timely care preserves both comfort and visual function.
At Next Level Retina patients receive a focused clinical assessment that includes a detailed history, slit-lamp examination and photographic documentation when indicated to track changes over time. The evaluation emphasizes identifying modifiable risk factors such as UV exposure and dry eye, distinguishing benign pterygia from lesions that warrant biopsy, and developing an individualized plan that balances conservative care with timely intervention when appropriate. When surgery is recommended, the team discusses grafting options and postoperative expectations to minimize recurrence and preserve ocular surface health.
Dr. Neel Lamba brings subspecialty expertise in retinal and ocular surface disease to the evaluation and coordinates care tailored to each patient's lifestyle and visual needs. Follow-up and preventive counseling, including UV protection and dry eye management, are integral parts of care to reduce progression and support long-term comfort and vision. Patients in the Oak Brook and greater Chicago area can expect clear explanations of findings and a treatment plan aligned with current best practices.
Phone:
Fax: